
Leg Issues: Cranial Cruciate Disease in Dogs
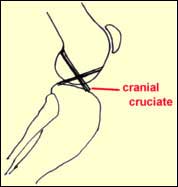
The knee is a fairly complicated joint. It consists of the femur above, the tibia below, the kneecap (or “patella”) in front, and the bean-like fabellae behind. Chunks of cartilage called the medial and lateral menisci fit between the femur and tibia like cushions and there are an assortment of ligaments holding everything together allowing the knee to bend the way it should and keep it from bending the way it shouldn’t.
First the Basics
 There are two cruciate ligaments that cross inside the knee joint: the anterior (or, more correctly in animals, “cranial”) cruciate and the posterior (or, more correctly in animals, the “caudal”) cruciate. They are named for the side of the knee (front or back) where their lower attachment is found. The anterior cruciate ligament prevents the tibia from slipping forward out from under the femur.
There are two cruciate ligaments that cross inside the knee joint: the anterior (or, more correctly in animals, “cranial”) cruciate and the posterior (or, more correctly in animals, the “caudal”) cruciate. They are named for the side of the knee (front or back) where their lower attachment is found. The anterior cruciate ligament prevents the tibia from slipping forward out from under the femur.
Finding the Rupture
The ruptured cruciate ligament is the most common knee injury of the dog; in fact, chances are that any dog with a sudden rear leg lameness has a ruptured anterior cruciate ligament rather than something else. The history usually involves a rear leg suddenly so sore that the dog can hardly bear weight on it. If left alone, it will appear to improve over the course of a week or two but the knee will be notably swollen and arthritis will set in quickly. Dogs can be present in either the acute stage (shortly after the injury) or in the chronic stage (weeks or months later).
The key to the diagnosis of the ruptured cruciate ligament is the demonstration of an abnormal knee motion called a “drawer sign.” It is not possible for a normal knee to show this sign.
The Drawer Sign
The veterinarian stabilizes the position of the femur with one hand and manipulates the tibia with the other hand. If the tibia moves forward (like a drawer being opened), the cruciate ligament is ruptured.
Another test that can be used is the “Tibial Compression test” where the veterinarian stabilizes the femur with one hand and flexes the ankle with the other hand. If the ligament is ruptured, again the tibia moves abnormally forward.
If the rupture occurred some time ago, there will be swelling on the side of the knee joint that faces the other leg. This is called a “medial buttress” and is a sign that arthritis is well along.
It is not unusual for animals to be tense or frightened at the vet’s office. Tense muscles can temporarily stabilize the knee preventing the demonstration of the drawer sign during the examination. Often sedation is needed to get a good evaluation of the knee. This is especially true with larger dogs. Eliciting a drawer sign can be difficult if the ligament is only partially ruptured so a second opinion with an orthopedic specialist is a good idea if the initial examination is inconclusive.
Since arthritis can set in relatively quickly after a cruciate ligament rupture, radiographs to assess arthritis are helpful. Another reason for radiographs is that occasionally when the cruciate ligament tears, a piece of bone where the ligament attaches to the tibia breaks off as well. This will require repair and the surgeon will need to know about it before beginning surgery. Arthritis present prior to surgery limits the extent of the recovery after surgery though surgery is still needed to slow or even curtail further arthritis development.
How the Rupture Happens
There are several clinical pictures seen with ruptured cruciate ligaments. One is a young athletic dog playing roughly who takes a bad step and injures the knee while playing. This is usually a very sudden lameness in a young large breed dog.
A recent study identified the following breeds as being particularly at risk for this phenomenon: Neapolitan mastiff, Newfoundland, Akita, St. Bernard, Rottweiler, Chesapeake Bay retriever, and American Staffordshire terrier.
On the other hand, an older large dog, especially if overweight, can have weakened ligaments and slowly stretch or partially tear them. The partial rupture may be detected or the problem may not become apparent until the ligament breaks completely. In this type of patient, stepping down off the bed or a small jump can be all it takes to break the ligament. The lameness may be acute but have features of more chronic joint disease or the lameness may simply be a more gradual/chronic problem.
Larger overweight dogs that rupture one cruciate ligament frequently rupture the other one within a year’s time. An owner should be prepared for another surgery in this time frame.
What happens if the Cruciate Rupture is not surgically repaired
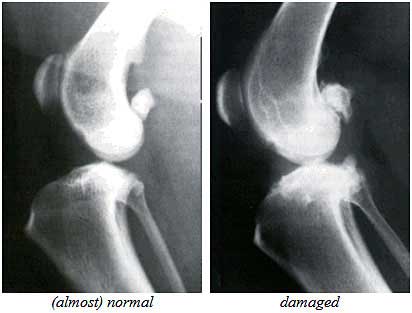
Without an intact cruciate ligament, the knee is unstable. Wear between the bones and meniscal cartilage becomes abnormal and the joint begins to develop degenerative changes. Bone spurs called “osteophytes” develop and chronic pain and loss of joint motion result. This process can be arrested by surgery but cannot be reversed.
- Osteophytes are evident as soon as 1-3 weeks after the rupture in some patients.
This kind of joint disease is substantially more difficult for a large breed dog to bear though all dogs will ultimately show degenerative changes. Typically, after several weeks from the time of the acute injury, the dog may appear to get better but is not likely to become permanently normal.
- In one study a group of dogs was studied for 6 months after cruciate rupture. At the end of 6 months, 85% of dogs under 30 lbs of body weight had regained near normal or improved function while only 19% of dogs over 30 lbs had regained near normal function. Both groups of dogs required at least 4 months to show maximum improvement.
What happens in surgical repair?
 There are 3 different surgical repair techniques commonly used, and a fourth method that has fallen out of favor in recent years:
There are 3 different surgical repair techniques commonly used, and a fourth method that has fallen out of favor in recent years:
Extracapsular Repair:
This procedure is currently favored as it can be performed in a relatively shorter surgery time than the other procedures and does not require specialized equipment. The knee joint is opened and inspected. The torn or partly torn cruciate ligament is removed. Any bone spurs of significant size are bitten away with an instrument called a “rongeur.” If the meniscus is torn, the damaged portion is removed. A large, strong suture is passed around the fabella behind the knee and through a hole drilled in the front of the tibia. This tightens the joint to prevent drawer motion, effectively taking over the job of the cruciate ligament.
- Typically, the dog may carry the leg up for a good 2 weeks after surgery but will increase knee use over the next 2 months eventually returning to normal
- Typically, the dog will require 8 weeks of exercise restriction after surgery (no running, outside on a leash only including the backyard)
- The suture placed will break 2-12 months after surgery and the dog’s own healed tissue will “hold” the knee.
Tibial Plateau Leveling Osteotomy (TPLO):
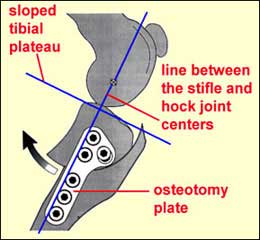 This procedure uses a fresh approach to the biomechanics of the knee joint and is meant to address the lack of success seen with the above technique long-term in larger dogs. With this surgery, the tibia is cut and rotated in such a way that the natural weight-bearing of the dog actually stabilizes the knee joint. As before the knee joint still must be opened and the damaged meniscus removed. The cruciate ligament remnants may or may not be removed depending on the degree of damage.
This procedure uses a fresh approach to the biomechanics of the knee joint and is meant to address the lack of success seen with the above technique long-term in larger dogs. With this surgery, the tibia is cut and rotated in such a way that the natural weight-bearing of the dog actually stabilizes the knee joint. As before the knee joint still must be opened and the damaged meniscus removed. The cruciate ligament remnants may or may not be removed depending on the degree of damage.
This surgery is complex and involves special training in this specific technique. Many radiographs are necessary to calculate the angle of the osteotomy (the cut in the tibia). At this time the TPLO is felt by many experts to be the best way to repair a cruciate ligament rupture regardless of the size of the dog and is especially appropriate for dogs over 50lbs. This surgery typically costs twice as much as the extracapsular method and requires a specialist.
- Typically, most dogs are touching their toes to the ground by 10 days after surgery although it can take up to 3 weeks.
- As with other techniques, 8 weeks of exercise restriction are needed.
- Full function is generally achieved 3 to 4 months after surgery and the dog may return to normal activity.
Tibial Tuberosity Advancement (TTA):

The TTA represents another take on how to use the biomechanics of the knee to create stabilization. The idea is that when the cruciate ligament is torn, the tibial plateau (the top of the tibia) and the patellar ligament should be repositioned at 90 degrees to one another to combat the shear force generated as the dog walks. To make this happen, the tibial tuberosity (front of the tibia where the patellar ligament attaches) is separated and anchored in its new position by a titanium or steel “cage,” “fork,” and plate. Bone grafts are used to assist healing. This procedure was developed in 2002 at the University of Zurich and since then over 20,000 patients worldwide have had this surgery. Some experts prefer it to the TPLO while others prefer the TPLO. Both procedures require specialized equipment and expertise.
- Typically the leg is bandaged for a week after surgery.
- The patient's activity must be restricted and confinement is a must post-operatively with gradually increasing activity over 3-4 months. Most dogs can return to normal activity 4 months after surgery.
Intracapsular Repair: (sometimes called the “over the top” method)

We mention this procedure for its historical significance though it is not one of the “big three.” This procedure has fallen out of favor lately as it has been unable to demonstrate results superior to those of the extracapsular technique described above though apparently, it is still a popular repair method in the U.K.
Intracapsular repair intuitively seems like it should do better as it uses living tissue (rather than an artificial material) to essentially make a new ligament. This takes more time surgically. As with the extracapsular repair, the knee joint is opened, and fragments of the ligament are removed, as is the damaged meniscus. After this, a strip of connective tissue is dissected locally and passed through the middle of the joint exactly where the cruciate ligament used to be. The “new ligament” is attached at the opposite end to an implant or simply sewn into place.
- Bandaging for a couple of weeks after surgery is commonly recommended.
- Again, the dog may not bear weight for a good two weeks after surgery and will likely require 2 months to return to normal function.
- Again, 8 weeks of exercise restriction will be necessary for healing.
General Rehabilitation after Surgery
Rehabilitation following the extracapsular repair method can begin as soon as the pet goes home. The area can be chilled with a padded ice pack for 10 minutes a couple of times daily. (Do not try to make up for a skipped treatment by icing the area longer; prolonged cold exposure can cause injury.) Passive range of motion exercise where the knee is gently flexed and extended can also help. It is important not to induce pain when moving the limb. Let the patient guide you. Avoid twisting the leg. After the stitches or staples are out (or after the skin has healed in about 10-14 days), water treadmill exercises can be used if a facility is available. This requires strict observation and, if possible, the patient should wear a life jacket. Walking uphill or on stairs is helpful for strengthening the back legs but no running, jumping, or other “explosive” type exercise should be performed for a full three months after surgery. Rehabilitation for patients with intracapsular repair is similar but slower in progression.
Rehabilitation after TPLO or TTA is gentler. Icing as above and rest are the main modes of therapy. After 3 to 4 weeks, an increase in light activity can be introduced. A water treadmill is helpful. No jumping, running, or stair-climbing is allowed at first. Expect the osteotomy site to require a good 6 weeks to heal.
What if the rupture isn’t discovered for years and joint disease is already advanced?
A dog with arthritis pain from an old cruciate rupture may still benefit from a TPLO surgery and possibly from the TTA. It may be worth having a surgery specialist take a look at the knee. Most cases must make do with medical management. Visit our section on arthritis treatment.
Meniscal Injury
 When the crucial ligament ruptures, the medial (on the inner side of the knee) meniscus frequently tears and must either be removed, partly removed, or ideally repaired. This is generally done at the time of cruciate ligament surgery and we would be remiss not to mention it.
When the crucial ligament ruptures, the medial (on the inner side of the knee) meniscus frequently tears and must either be removed, partly removed, or ideally repaired. This is generally done at the time of cruciate ligament surgery and we would be remiss not to mention it.
Pets with meniscal damage may have an audible clicking sound when they walk or when the knee is examined, but for a definitive diagnosis, the menisci must actually be inspected during surgery. It is difficult to access the menisci and thus repairing a tear in the meniscus is problematic; furthermore, poor blood supply to the menisci also makes good healing less likely. For these reasons, removal of the damaged portion of the meniscus is the most common surgical choice. This leaves some meniscus behind to distribute the compression load on the knee but removes the painful, ineffective portion.
Areas of current research include techniques to improve blood supply to the healing meniscus so that repair can be more feasible. If meniscal damage has occurred in a cruciate rupture, arthritis is inevitable and surgery should be considered a palliative procedure.